
Translate this page into:
Latest reviews regarding COVID-19 and its management
-
Received: ,
Accepted: ,
How to cite this article: Hossain MI, Raghunath CN. Latest reviews regarding COVID-19 and its management. Karnataka Paediatr J 2020;35(1):23-8.
Abstract
We discuss briefly regarding the origin of the SARS-CoV-2 virus, it’s structure, routes of transmission, and pathophysiology. Then, we go on to describe the symptomatology and clinical features based on different publications from different countries. Finally, we have summarized the variable guidelines available for the management and prevention of the COVID-19 disease.
Keywords
COVID-19
Corona
Corona in children
Management of Corona
Effect of corona in children

Coronavirus (CoV) is not a new virus. It is a large family of virus which has been causing different diseases such as common cold to Middle East respiratory syndrome (MERS-CoV) and severe acute respiratory syndrome (SARS-CoV)
Almost all viruses causing common cold go through genetic mutation and form new strains. Same way, the current coronavirus called SARS-CoV2 is a new strain that causes COVID-19 disease and bat appears to be the reservoir but the intermediate host(s) is unknown.[1]
Coronaviruses are zoonotic. Detailed investigations found that SARS-CoV transmitted from civet cats to humans and MERS-CoV came from dromedary camels.[2] There are more coronaviruses which are circulating in animals that have not yet infected humans.
SARS-CoV-2 viruses like other coronaviruses, are spherical, containing single-stranded RNA and have protein spikes protruding from their surface called spike protein [Figure 1]. These spikes latch onto human cells and undergo a structural change that allows the viral membrane to fuse with the host’s cell membrane. The viral genes can then enter the host cell to be copied, producing more viruses.[3]
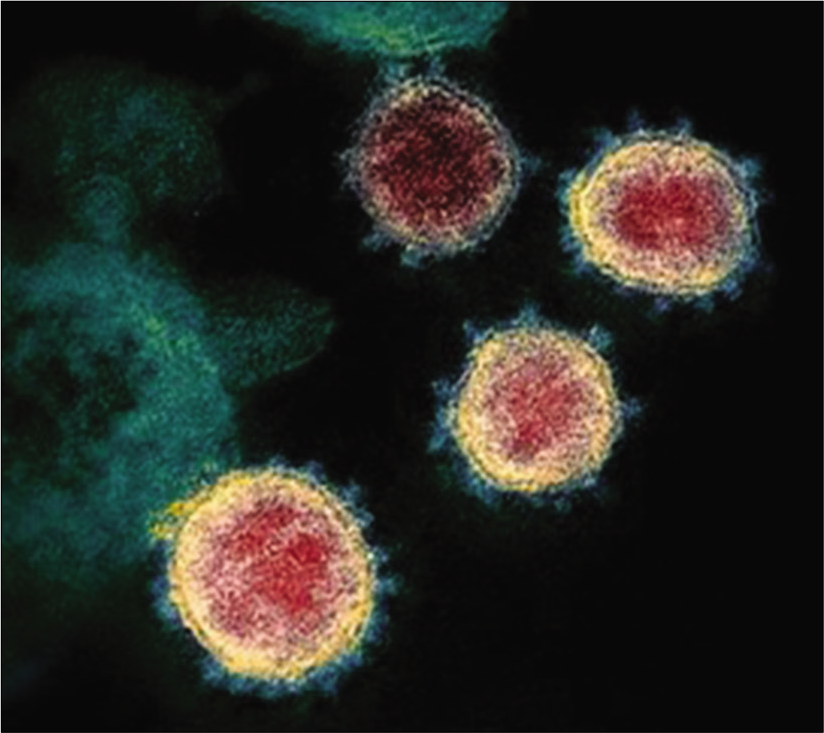
- Transmission electron microscope image shows SARS-CoV-2.[3]
Latest work shows that, like the virus that caused the 2002 SARS outbreak, SARS-CoV-2 spikes bind to angiotensin-converting enzyme 2 (ACE2).[3]
SARS-CoV-2 spike is 10–20 times more likely to bind ACE2 which might be the reason why they are more infectious than the previous strains of CoV.[3]
Even though the structure of latest strains of virus is similar to SARS-CoV, three known antibodies against SARS-CoV could not bind to SARS-CoV2, which indicates that the treatment with antibodies of SARS-CoV is unlikely to be successful.[3]
ROUTES OF TRANSMISSION
COVID-19 virus is transmitted through droplets and fomites, therefore, transmission can occur by direct contact with infected people and indirect contact with surfaces in the immediate environment or with objects used on the infected person (e.g., stethoscope or thermometer).[4]
Airborne transmission may be possible during procedures or support treatments that generate aerosols; that is, endotracheal intubation, bronchoscopy, open suctioning, administration of nebulized treatment, manual ventilation before intubation, turning the patient to the prone position, disconnecting the patient from the ventilator, non-invasive positive pressure ventilation, tracheostomy, and cardiopulmonary resuscitation.[4]
Prolonged (up to a month) fecal shedding of viable virus has been identified in a limited number of case reports, but feco-oral route of transmission has not been reported to date.[4,5]
Vertical transmission of COVID-19 to infant during delivery or breastfeeding remains to be confirmed.[6]
INCUBATION PERIOD
Incubation period varies from 1 to 14 days; mean period being 5–6 days.
CHILDREN
Limited data available in India regarding COVID-19 in children show that the prevalence of the disease is around 2% which corresponds to reports from other countries.
According to Joint Commission by China and CDC, COVID-19 seems to be rare and mild in individuals aged <18 years (2.4%) and out of these patients, only 2.5% developed severe and 0.2% went on to have critical disease.[1]
According to CDC report of the U.S. cases, 2% were of pediatric age group.[5,7]
In Italy, 1.2% of COVID-19 cases were among the age group of <18 years.[8]
PATHOPHYSIOLOGY
ARDS
The primary pathology is characterized by diffuse alveolar damage through hyperinflammatory and direct effect of the virus activity.[9]
Cytokine storm
New evidences suggest that some patients respond to SARS- CoV2 with cytokine storm-like sepsis and HLH.[10]
THE SIGNS AND SYMPTOMS
Symptoms are non-specific and it can range from being asymptomatic to severe pneumonia and death [Table 1 and Figure 2].
| Sign/symptom | No. (%) with sign/symptom | |
|---|---|---|
| Pediatric | Adult | |
| Fever, cough, or shortness of breath | 213 (73) | 10,167 (93) |
| Fever | 163 (56) | 7794 (71) |
| Cough | 158 (54) | 8775 (80) |
| Headache | 81 (28) | 6,335 (58) |
| Sore throat | 71 (24) | 3,795 (35) |
| Myalgia | 66 (23) | 6713 (61) |
| Shortness of breath | 39 (13) | 4674 (43) |
| Diarrhea | 37 (13) | 3353 (31) |
| Nausea/vomiting | 31 (11) | 1746 (16) |
| Runny nose | 21 (7.2) | 757 (6.9) |
| Abdominal pain | 17 (5.8) | 1329 (12) |
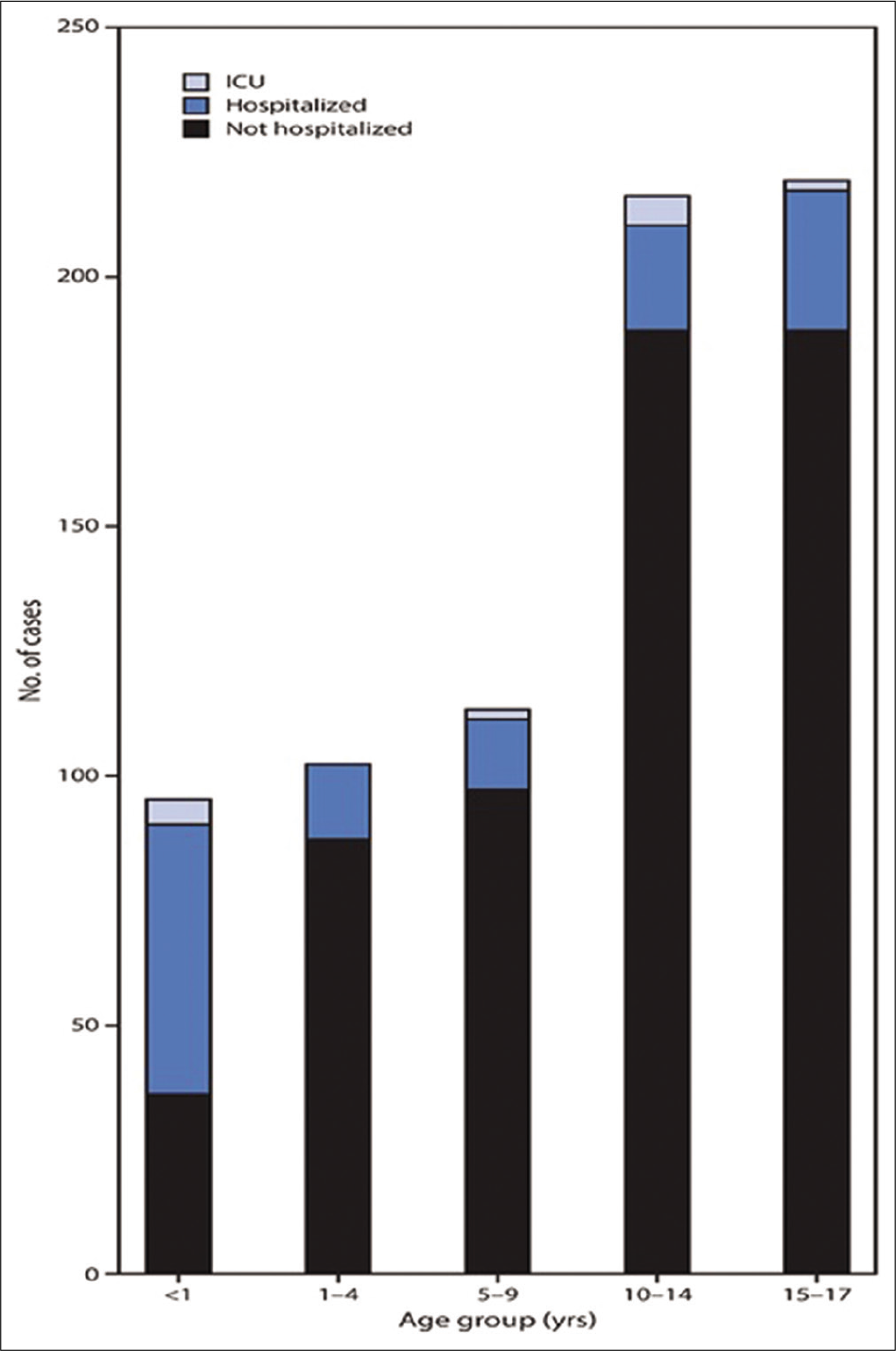
- COVID-19 cases among children aged <18 years, among those with known hospitalization status (N = 745), †by age group and hospitalization status – United States, February 12–April 2, 2020.[7] †Number of children missing hospitalization status by age group: <1 year (303 of 398; 76%); 1–4 years (189 of 291; 65%); 5–9 years (275 of 388; 71%); 10–14 years (466 of 682; 68%); 15–17 years (594 of 813; 73%).
Some children present in shock and with typical/ atypical features of Kawasaki disease, which is a vascular inflammatory disease.
SEVERITY OF DISEASE
Asymptomatic
Mild-to-moderate disease: It includes non-pneumonia and mild pneumonia cases.[1]
Severe disease: Categorized by dyspnea, respiratory distress, blood oxygen saturation ≤93%, PaO2/FiO2 ratio <300, and/or lung infiltrates >50% of the lung field within 24–48 h.[1]
Critical: Respiratory failure, septic shock, and/or multiple organ dysfunction/failure.[1]
High risk for severe and critical disease in younger age is underlying pulmonary pathology, immunocompromising conditions, obesity, and coinfection.[5]
Pregnant women (8% had severe disease and 1% were critical): Risk of severity of the disease in pregnant and non-pregnant women of similar age appears to be equal.[1]
APPROACH TO DIAGNOSIS AND TREATMENT
History of epidemiology
Travel or residence history in containment zone and its surrounding areas or other communities with reported cases within 14 days before the onset of the disease.
History of contact with SARS-CoV2-positive patients within 14 days before the onset of the disease.
Contact with patients with fever or respiratory symptoms from containment zone and its surrounding areas or other communities with reported cases within 14 days before the onset of the disease.
Cluster infection: Within 2 weeks, 2 or more cases of fever, and/or respiratory symptoms occurred in small areas such as homes, offices, and school classes.
Clinical manifestations and laboratory findings
Fever and/or respiratory symptoms
-
Having the imaging features of COVID-19:
The total leukocyte count is normal or decreased, or the lymphocyte count is normal or decreased in the early stage of the disease.[10,11]
They can have normal platelet count or thrombocytosis.
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are elevated, while procalcitonin is normal in adults, it may be elevated in pediatric patients.[11]
Some patients have an increase in liver enzymes, lactate dehydrogenase (LDH), muscle enzymes, and myoglobin.
Elevated troponin is seen in some critically ill patients.
In severe cases, D-dimer increases and peripheral blood lymphocytes progressively decrease.
Severe and critically ill patients often have elevated inflammatory factors.
-
Some present with multisystem inflammatory syndrome in children (MIS-C):[12]
Defined by fever >24 h, laboratory evidence of inflammation, and evidence of clinically severe illness requiring hospitalization, with multisystem (≥2) organ involvement (cardiac, renal, respiratory, hematologic, gastrointestinal, dermatologic, or neurological); AND
No alternative plausible diagnosis; AND
Positive for current or recent SARS-CoV-2 infection by RT-PCR, serology, or antigen test; or COVID-19 exposure within the 4 weeks before the onset of symptoms
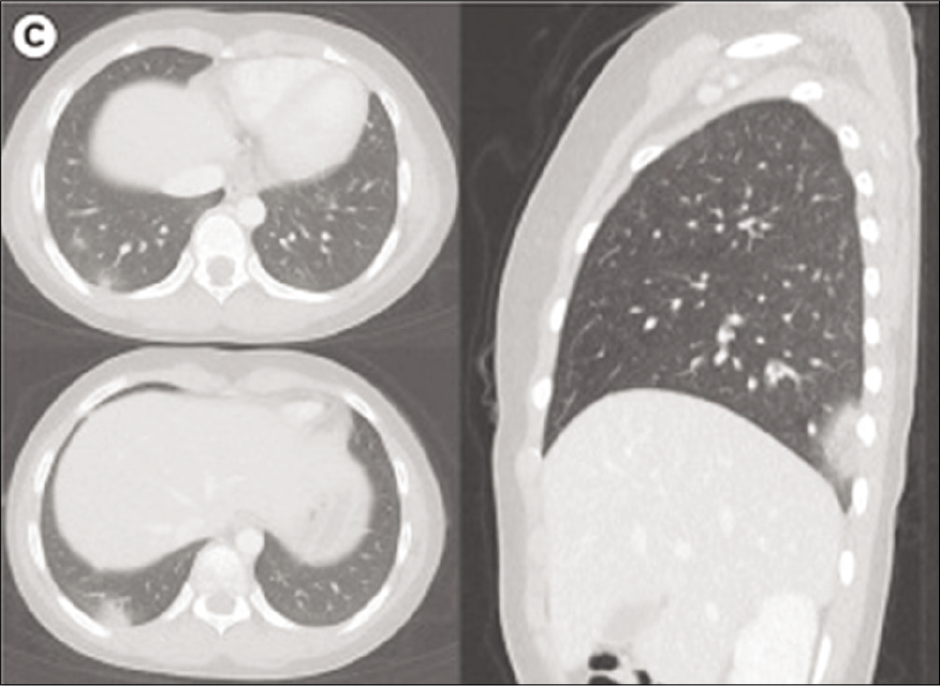
- (C) Chest CT performed on the fourth day since symptom onset demonstrates patchy nodular consolidations with peripheral ground glass opacities in subpleural areas of the right lower lobe in axial and sagittal views of CT.[15]
Some individuals may fulfill full or partial criteria for Kawasaki disease but should be reported if they meet the case definition for MIS-C.
Diagnosis of COVID-19
Is confirmed when suspected case with one of the following serological evidences:
Serum IgM antibodies and IgG antibodies to SARS- CoV2 are positive; serum IgG antibodies to SARS-CoV2 turn from negative to positive or the IgG antibody titers of recovery period are 4 times or more higher than that of acute phase.[13,14]
The result of virus gene sequencing analysis is highly homologous with the known SARS-CoV2.[13,14]
PREVENTION
-
Practice good personal hygiene:
Cover mouth and nose with a tissue when coughing or sneezing.
Wash hands frequently.
Do not touch mouth, eyes, and nose with dirty hands, and do not spit on the ground.
Avoid family gatherings and eat separately, as during meal everyone, are in close contact.
Avoid public places as much as possible.
Keep house well ventilated and sunlit.
Wear a mask if you have cold, cough, or fever. Consult a doctor and mention about travel history or if you have come across any individual who is suspected to have COVID-19 or diagnosed with COVID-19 in the past 14 days.[13]
TREATMENT
Confirmed and suspected cases should be isolated and treated in designated hospitals with effective isolation and protective conditions, and suspected cases should be isolated in separate rooms.
Self-isolation in pediatric age group is difficult. Considering the circumstances, the Korean Centers for Disease Control and Prevention and the Korean Society of Pediatric Infectious Diseases recommend one of the family members to be assigned as a caregiver for infants and young children who are suspected or confirmed with COVID-19, and the caregiver should take adequate measures to avoid being exposed to the virus. Thus, further pediatric-specific guidelines on the isolation and adequate personal protective equipment for caregivers should be prepared.[15]
Multiple confirmed cases can be admitted in the same ward, and critical cases should be shifted to ICU as soon as possible.
General treatments: Patients should be on bed rest, monitor vitals, connect them to pulse oximeter to monitor oxygen saturation, keep them well hydrated without causing fluid overload, prevent electrolyte imbalance, hourly visits to look out for respiratory distress and importantly, should receive adequate nutrition.
Complete blood count, urinalysis, CRP, biochemical indicators (liver enzyme, myocardial enzyme, renal function, etc.), blood coagulation function, arterial blood gas analysis, and chest imaging should be investigated according to the conditions of the patients.
Cytokines testing can be done if available.
Effective oxygen therapy measures should be provided in time, using nasal cannula, oxygen masks, and high- flow nasal cannula oxygen therapy.
Early intubation and protective mechanical ventilation are recommended and make sure closed tracheal aspiration systems are used.[16]
NIV to be avoided due to high risk of aerosol dispersion.[16]
Treatment with nitric oxide and/or sildenafil (0.5–2 mg/kg/dose Q4–6 h with a maximum of 20 mg/dose Q8 hours) for patients with persistent hypoxemia.[16]
ECMO
ANTI-VIRUS TREATMENT
Hydroxychloroquine/chloroquine (5–10 mg/kg/day of basic chloroquine for 10 days) and azithromycin (10 mg/kg on the 1st day, followed by 5 mg/kg/day for 4 days with a maximum dose of 30 mg/kg or 1500 mg).[16]
Antiviral agents, such as oseltamivir, ribavirin, ganciclovir, remdesivir, lopinavir, and ritonavir, have been used to reduce the viral load to prevent potential respiratory complications without any success.[16]
IMMUNOMODULATORY TREATMENT IN CHILDREN WITH COVID-19
Glucocorticoids to be considered in patients with COVID-19 and hyperinflammation.[17]
Anakinra at >4 mg/kg/day I.V/S.C is found to be safe in severe infection and maybe be beneficial if administered before invasive ventilation.
Tocilizumab (<30 kg: 12 mg/kg IV; >30 kg: 8 mg/kg IV, max: 800 mg) may be effective in reducing the mortality. It may increase risk of bacterial and fungal infection.[17,18]
ANTIPLATELET AND ANTICOAGULATION THERAPY IN MIS-C
Low-dose aspirin (3–5 mg/kg/day; max 81 mg/day) in MIS-C and KD-like features and/or thrombocytosis (platelet count ≥450,000/μL) and continued until normalization of platelet count and confirmed normal coronary arteries at ≥4 weeks after diagnosis. Contraindicated in patients with a platelet count ≤80,000/μL.[17]
Children with dilated coronary artery are recommended to receive enoxaparin at therapeutic dose along with low dose of aspirin.[17]
For MIS-C patients who do not meet the mentioned criteria should have a tailored antiplatelet and anticoagulation therapy based on risk for thrombosis.[17]
IMMUNOMODULATORY TREATMENT IN MIS-C
High-dose IVIG (typically 1–2 g/kg) is recommended for the treatment of MIS-C. Cardiac function and hydration status should be checked before IVIG administration. IVIG to be administered when cardiac function is restored.[17]
Low-moderate-dose glucocorticoids to be considered for the treatment of MIS-C. High-dose, IV pulse glucocorticoids may be considered to treat patients with life-threatening complications, such as shock, especially refractory shock.[17]
Anakinra (IV or SQ) can be considered for the treatment of MIS-C refractory to IVIG and glucocorticoids or in patients with contraindications to these treatments.[17]
DISCHARGE CRITERIA
-
Clinical recovery:
Afebrile >3 days,
Resolution of symptoms and radiologic improvement.
Two negative PCR tests taken 24 h apart.[14]
PROGRESSION OF DISEASE
From the data available, the average time taken from the onset of disease to clinical recovery for mild cases is approximately 2 weeks, while it is 3–6 weeks for patients with severe or critical disease.[14]
Onset of severe disease from initial symptoms, including hypoxia, is 1 week.[14]
Among patients who have died, the duration of the disease ranges from 2 to 8 weeks.[14]
Early identification of cases and contacts allows for earlier treatment and better recovery.
PROGNOSIS
Symptoms in infected children are relatively mild.
According to the cases currently treated, most of the patients have a good prognosis and a few are in severe condition.
The prognosis of the elderly and patients with chronic underlying diseases is relatively poor.\
Prognosis of COVID-19 in pregnant and non-pregnant women of similar age appears to be equal.[14]
RECOMMENDATIONS AFTER DISCHARGE
After discharge, it is advised to continue to monitor self- health for 2 weeks, wear mask, and if possible, live in a single room with adequate ventilation.
Avoid close contact with family members, eat separately, keep hands clean, and avoid outdoor activities.
Go to the hospital for a follow-up visit at the 2nd and 4th weeks after discharge or at the onset of recurrence of any symptoms.[14]
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) 2020. Geneva: World Health Organization; Available from: https://www.who.int/docs/default-source/coronaviruse/whochina-joint-mission-on-covid-19-final-report.pdf [Last accessed on 2020 Feb 24]
- [Google Scholar]
- The battle against SARS and MERS coronaviruses: Reservoirs and animal models. Anim Model Exp Med. 2018;1:125-33.
- [CrossRef] [PubMed] [Google Scholar]
- Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020;367:1260-3.
- [CrossRef] [PubMed] [Google Scholar]
- Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations Geneva: World Health Organization; 2020.
- [Google Scholar]
- COVID-19 in children: Initial characterization of the pediatric disease. Pediatrics. 2020;145:e20200834.
- [CrossRef] [PubMed] [Google Scholar]
- An Analysis of 38 pregnant women with COVID-19, their newborn infants, and maternal-fetal transmission of SARS-CoV-2: Maternal coronavirus infections and pregnancy outcomes. Arch Pathol Lab Med. 2020;2020:5858.
- [CrossRef] [PubMed] [Google Scholar]
- Coronavirus disease 2019 in children-United States February 12-April 2 2020. MMWR Morb Mortal Wkly Rep. 2020;69:422-6.
- [CrossRef] [PubMed] [Google Scholar]
- Coronavirus Disease 2019 (COVID-19) in Italy. JAMA. 2020;323:1335.
- [CrossRef] [PubMed] [Google Scholar]
- Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-2.
- [CrossRef] [Google Scholar]
- Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-8.
- [CrossRef] [Google Scholar]
- Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect Dis. 2020;20:689-96.
- [CrossRef] [Google Scholar]
- Distributed Via the CDC Health Alert Network.CDCHAN-00432. 2020. Centers for Disease Control and Prevention. Available from: https://www.emergency.cdc.gov/han/2020/han00432.asp [Last accessed on 2020 May 14]
- [Google Scholar]
- Diagnosis and Treatment Protocol for COVID-19 (Trial Version 7) (6th ed). China: General Office of the National Health Commission and the Office of the National Administration of Traditional Chinese Medicine; 2020.
- [Google Scholar]
- Diagnosis and treatment protocol for COVID-19 (Trial Version 7) the general office of the national health commission and the office of the national administration of traditional Chinese medicine In: PUMCH COVID-19 Prevention and Precautions Handbook. Chinese: Academy of Medical Sciences and Peking Union Medical College Hospital; 2020.
- [Google Scholar]
- First pediatric case of coronavirus disease 2019 in Korea. J Korean Med Sci. 2020;35:e124.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 Diagnostic and management protocol for pediatric patients. Clinics (Sao Paulo Brazil). 2020;75:e1894.
- [CrossRef] [PubMed] [Google Scholar]
- American college of rheumatology clinical guidance for pediatric patients with multisystem inflammatory syndrome in children (MIS-C) associated with SARS-CoV-2 and Hyperinflammation in COVID-19 Version 1. Arthritis Rheumatol. 2020;2020:41454.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19: Informal Consultation on the Potential Role of IL6/IL-1 Antagonists in the Clinical Management of COVID 19 Infection Geneva, Switzerland: WHO R&D Blueprint; 2020.
- [Google Scholar]




