
Translate this page into:
Leigh like phenotype secondary to 3-hydroxyisobutyryl-CoA hydrolase deficiency: A first Indian case
*Corresponding author: Vykuntaraju K. Gowda, Department of Pediatric Neurology, Indira Gandhi Institute of Child Health, Bengaluru, Karnataka, India. drknvraju08@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gowda VK, Srinivasan VM, Reddy VS, Nayyer A. Leigh like phenotype secondary to 3-hydroxyisobutyryl-CoA hydrolase deficiency: A first Indian case. Karnataka Paediatr J. 2024;39:70-1. doi: 10.25259/KPJ_9_2024.
Dear Editor,
Biallelic mutations in the 3-hydroxyisobutyryl-CoA hydrolase (HIBCH) gene causes HIBCH deficiency (HIBCHD) (HIBCHD: OMIM#250620) and present with neurodegeneration, psychomotor retardation, lactic acidosis and abnormalities of basal ganglia.[1] We are reporting a case of HIBCHD presenting as Leigh phenotype.
A 16-month-old male born to consanguineous parentage presented with developmental delay followed by regression, stiffness of limbs, and encephalopathy. Developmentally, attained partial neck controls from 8 months, roll over at 12 months, monosyllables by 13 months, social smile by 6 months, and recognition of mother by 7 months. At around 15 months of age, following febrile illness, the child lost all attained milestones and developed stiffness of limbs. On examination, the occipitofrontal circumference was 44 cm (−1.36 Z score), weight was 8.35 kg (−1.34 Z score), hypertonia with intermittent dystonia, power of 4/5 and exaggerated deep tendon reflexes with extensor plantar response [Figure 1a]. Tandem mass spectrometry (TMS) screening showed elevated C4 hydroxyl carnitine (1.42: Normal range: 0–0.50: NMT - 5.56). Magnetic resonance imaging revealed bilateral symmetrical T2 hyperintensities involving globus pallidus, diffuse cerebral atrophy, and thin corpus callosum with diffusion restriction in bilateral globus pallidus, with hyperintensity on diffusion-weighted images and hypointensity of corresponding apparent diffusion coefficient maps. Small cystic changes representing necrosis were noted in bilateral globus pallidus [Figure 1b-f]. Exome sequencing was sent in suspicion of Leigh like syndrome and identified a novel frameshift deletion c.131delG, p.(Gly44fs*6) in exon-3 of the HIBCH gene. The variant is classified as likely pathogenic as per ACMG classification.
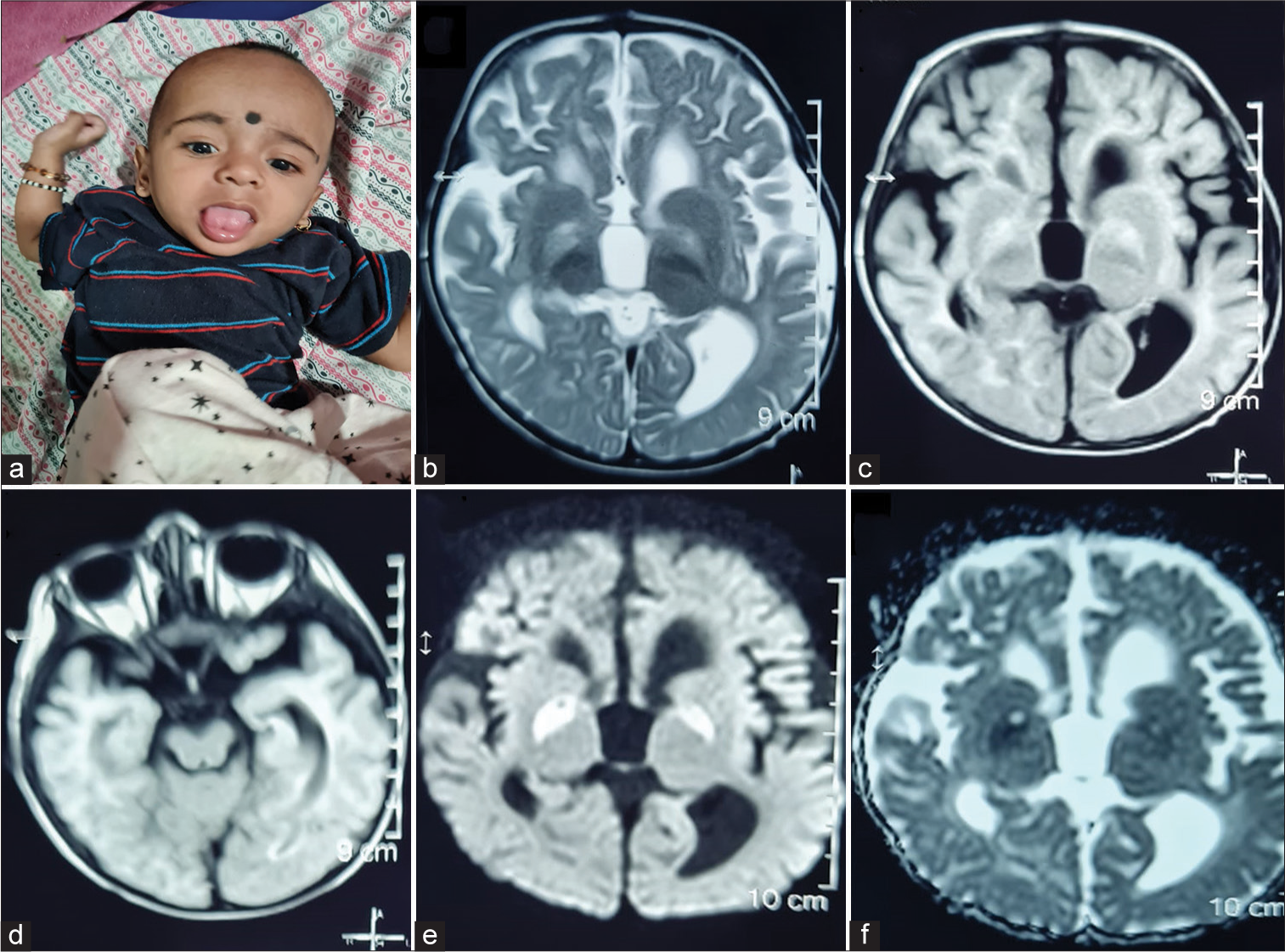
- (a) Clinical photograph of the child showing tongue and upper limb dystonia, (b) axial T2-weighted (Two headed arrow), (c) fluid-attenuated inversion recovery sequences of magnetic resonance imaging of brain images showing bilateral symmetrical globus pallidus hyperintensity, bilateral basal ganglia atrophy, predominantly involving globus pallidus (left more than right) (Two headed arrow), (d) cerebral peduncles appear normal (Two headed arrow), (e) axial diffusion weighted images (DWIs) (Two headed arrow) show restriction of diffusion in bilateral globus pallidus, with hyperintensity on DWI images and (f) hypointensity of corresponding apparent diffusion coefficient maps (Two headed arrow).
The HIBCHD presents with developmental delay, dystonia clinically, and basal ganglia involvement radiologically.[1] Biochemically, the elevation of hydroxy C4 carnitine and urinary excretion of methacrylyl CoA metabolites and S2 carboxy propyl cysteine is found.[2] In the current case, we found elevation of C4 hydroxyl carnitine on TMS. The differentials considered were mitochondrial disorder, mainly Leighs and Leigh like syndrome, and short-chain enoyl CoA hydratase deficiency (ECHS1 mutation). There was a significant improvement in development and dystonia with dietary management with a low protein diet, symptomatic therapy, carnitine supplements and rehabilitation. To conclude, we report the first Indian child with HIBCH deficiency presenting as Leigh like syndrome.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- HIBCH mutations can cause Leigh-like disease with combined deficiency of multiple mitochondrial respiratory chain enzymes and pyruvate dehydrogenase. Orphanet J Rare Dis. 2013;8:188.
- [CrossRef] [PubMed] [Google Scholar]
- Metabolite studies in HIBCH and ECHS1 defects: Implications for screening. Mol Genet Metab. 2015;115:168-73.
- [CrossRef] [PubMed] [Google Scholar]




