
Translate this page into:
Focal areas of signal intensity in neurofibromatosis type 1(NF1)
*Corresponding author: Vykuntaraju K. Gowda, Department of Pediatric Neurology, Indira Gandhi Institute of Child Health, Bengaluru, Karnataka, India. drknvraju08@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gowda VK, Kinhal UV, Srinivasan VM, Saini J. Focal areas of signal intensity in neurofibromatosis type 1(NF1). Karnataka Paediatr J. 2025;40:38-9. doi: 10.25259/KPJ_40_2024
Dear Editor,
A 5-year-old girl presented with developmental delay and skin lesion with a history of similar skin lesions in her paternal grandmother. On examination, a child was hyperactive; multiple café-au lait macules with sizes ranging from subcentimetric to the largest one encircling the back, the left side of the trunk, and the abdomen measuring about 20 cm are shown [Figure 1a]. Lisch nodules in the iris of the right eye were noted. Magnetic resonance imaging of the brain showed multiple hypointense areas on T1-weighted images [Figure 1b] and hyperintensities on T2-weighted (T2W) images [Figure 1c-e] in the midbrain, bilateral lentiform nucleus, and medial temporal lobes. Sagittal T2W images of the brain and orbit [Figure 1f] showed thickened bilateral optic nerves, chiasma, and proximal optic tracts iso- to hypointense to brain parenchyma. An autosomal dominant, pathogenic frameshift deletion mutation of neurofibromatosis type 1 (NF1) gene at exon 12 was detected, confirming the diagnosis of NF1.
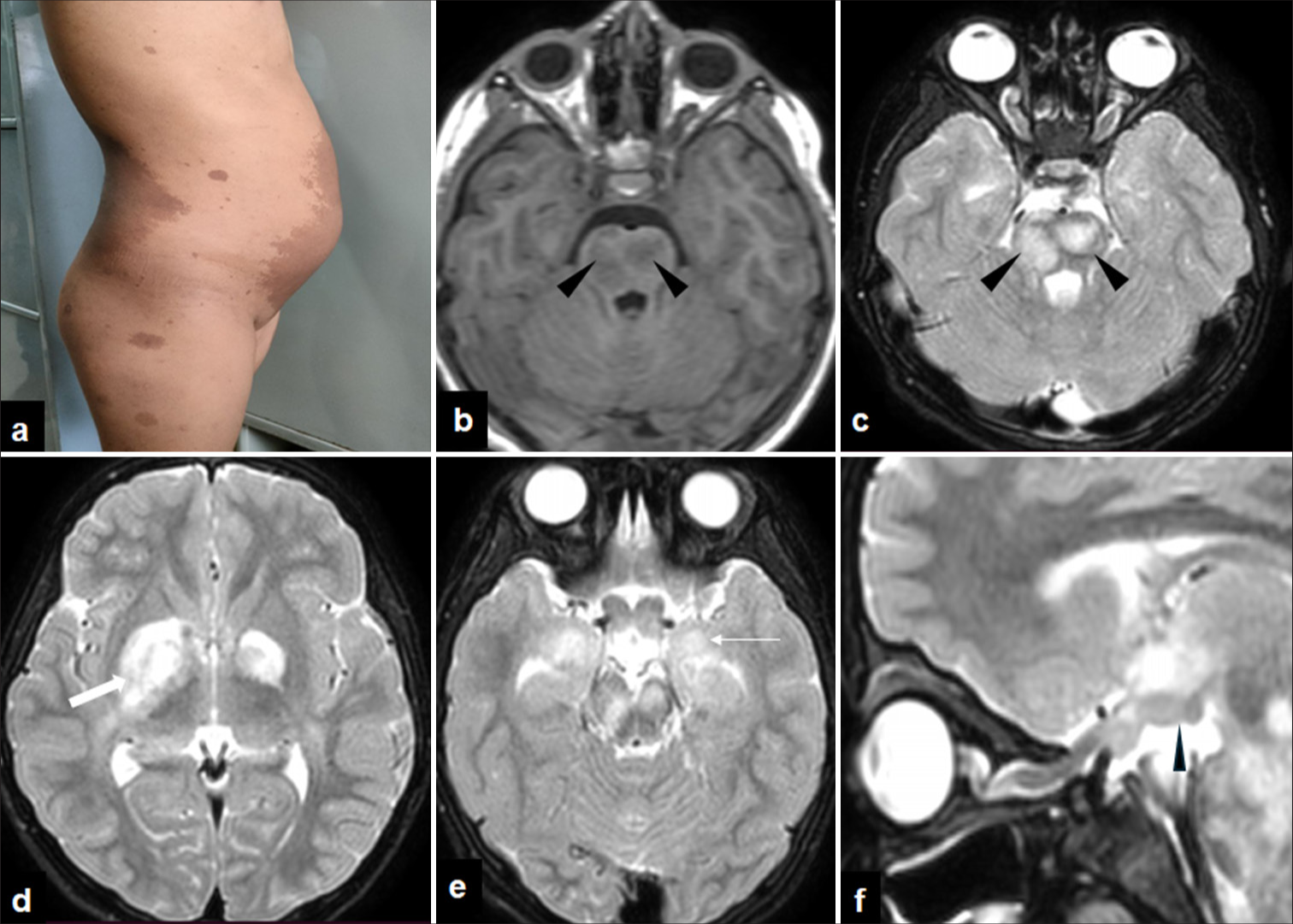
- (a) Clinical photograph of child showing multiple café-au lait macules, well circumscribed, dark brown pigmented skin lesions with sizes ranging from sub centimetric to largest one encircling back, left side of trunk and abdomen measuring about 20 cm. (b) Magnetic resonance imaging of axial T1-weighted images of the brain showing multiple hypointense areas in the midbrain (black arrow heads). (c) Axial T2-weighted (T2W) images of brain show multiple focal hyperintense lesions at brain stem (black arrow heads), (d) bilateral lentiform nucleus (thick white arrow) and (e) medial temporal lobes (thin white arrow). (f) Sagittal T2W images of brain and orbit shows thickened optic nerves, chiasma, and proximal optic tracts (black arrowhead) arrowhead iso- to hypointense to brain parenchyma.
The common neuroimaging feature noted in NF1 includes focal areas of signal intensity (FASI). The FASIs include T2 WI and fluid-attenuated inversion recovery hyperintensities with T1 iso/mild hyperintensities with no mass effect/ enhancements.[1] The differential diagnosis considered was demyelinating disorder and brain tumours. The demyelinating lesions are smaller than FASIs and show mass effect/surrounding oedema.[2] Tumours may be considered if the lesions show both clinical and radiological progression, mass effect, and magnetic resonance spectroscopy shows choline peak.[3] To differentiate FASI from optic glioma following points are to be considered: in FASI, no mass effect and contrast enhancement are seen compared to optic glioma. FASI is more commonly seen in optic chiasma and optic tract, and gliomas can be seen in the intraorbital part of the optic nerve as well as the optic chiasma and tracts.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Neuroimaging findings in neurofibromatosis type 1 and 2. Neuroimaging Clin N Am. 2004;14:149-70, vii
- [CrossRef] [PubMed] [Google Scholar]
- MRI in neurofibromatosis 1. The nature and evolution of increased intensity T2-weighted lesions and their relationship to intellectual impairment. J Neurol Neurosurg Psychiatry. 1993;56:492-5.
- [CrossRef] [PubMed] [Google Scholar]
- Serial MR imaging and 1H-MR spectroscopy of unidentified bright objects in a case of neurofibromatosis type 1. Brain Dev. 2005;27:595-7.
- [CrossRef] [PubMed] [Google Scholar]




